Over the last year, the resurgence of the Black Lives Matter movement has been paralleled by an accelerating movement to decolonise development. Among the many papers and blogs, this Lancet Perspectives article is one of the best. Seye Abimbola and Madhu Pai not only highlight the colonialist roots of global health, they go on to envision a decolonised future where equity, justice, humility and respect replace supremacy.
Supremacy goes well beyond ‘pale, male and stale’. It manifests in what does (or does not) happen between countries, and groups and individuals within those countries.
In research, it governs who sets the research question, who pays for the work, who decides on methods, who does the work, whose names are on the paper, who publishes it, who reads it and who decides on the next study to be done – or the next research program to be set up and funded. In a word, everything.
Much of the impetus on decolonisation in recent years has come from global health thinkers and doers like Abimbola and Pai, as the reading list below shows. But of course it transcends any one discipline. Last week, Arvind Subramanian and Devesh Kapur wrote about absent voices in development economics. They cited Kazuo Ishiguro’s 2017 Nobel lecture in which he urged the broadening of “our common literary world to include many more voices from beyond our comfort zones of the elite first-world cultures.”
The decolonisation movement has shone a light on questions of agency, power, human rights, equity and justice in the midst of a pandemic which has also brought these issues to the fore. Not only has COVID-19 exposed different forms of inequity, it has amplified them. People who are poor, marginalized and exploited are more likely to be dependent on fragile livelihoods that cannot be outsourced to Zoom meetings. It has led to the loss of livelihoods and lives.
The word ‘crisis’ comes from the Greek noun ‘krisis’ which means ‘to separate, decide….a turning point’
A year ago, Erica Nelson, Nick Nisbett and I decided to look into this potential ‘turning point’ in the light of past histories of global nutrition. Like global health, global nutrition has roots in colonialism and supremacy. We like to repeat the mantra that nutrition is both a marker (of deprivation) and a maker (of development) but we are far less likely to hark back to a history when nutrition was a discipline that propped up colonialism, racism, inequality and injustice.
Nutrition has always operated at the interface of health and food systems which have deep roots in colonialism. For global nutrition to move forward, it needs to confront its shady past – the overt and disguised racism, the systems of food apartheid and the massive power imbalances within health and food systems. Vaccine nationalism, global food trade terms are just two examples — there are many more.
Credit: Martin Karumwa
Twenty years ago, just after I joined IFPRI, I worked on ‘strengthening capacity for nutrition’. At that time the finger of blame for the failure of large-scale nutrition programs often pointed to insufficient/unsustainable capacities within communities and organizations responsible for implementing them.
But many of us then failed to take the next step. Inadequate capacity is not just the cause of failure, it’s the symptom of a larger failure that has its roots in colonisation and intergenerational injustice. The proper response to capacity gaps or weaknesses is not simply to initiate a capacity development program – it is to dig deeper, to respect, protect and fulfil the human right to food and health, and to work towards intergenerational equity and justice.
A recent article in the New Humanitarian shows how much work remains to be done. The EU’s commissioner for crisis management recently stated: “What is actually the biggest barrier to localisation is the capacity of local actors. Most often, the local organisations lack the capacity to fulfill all the criteria with regard to accountability, transparency, sound financial management…”
Just as ‘community-based’ does not equate with ‘community-driven’, localisation — defined and driven by global northern organisations — is far from decolonisation.
For those of us in the global north, decolonisation requires us to get out of the way – or ‘lean out’. It requires us to become better allies and enablers, not leaders.
The UNFSS promotes itself as a ‘people’s summit’ where everyone is welcome at the table. Current past UN human rights commissioners have written: “Coming to the table to discuss ‘solutions’ is not as simple as it sounds. What if the table is already set, the seating plan non-negotiable, the menu highly limited?” In their Lancet article, Abimbola and Pai also remind us, in a broader context, that “what is on the table is as important as who is around the table.”
In a seminar last week, the UN Secretary General’s Special Envoy, Agnes Kalibata provided assurances that human rights will be foundational to UNFSS processes, and that corporate capture is not an issue.
The big question remains – how will such an open-door policy address the huge power asymmetries between actors that underpin and enable dysfunctional food systems? If human rights are foundational to the Summit process and deliberations, then issues of power, agency and justice must be ‘on the table’ too. As far as I can see, there has been little open public discussion of these issues. Without this, the notion of transformation based on ‘game changers’ is meaningless.
In our brief review of global nutrition histories, we concluded that it is not enough to listen to different perspectives, we have to learn from them, and act differently as a result. To dig deeper, well below the surface to better understand the ‘causes of the causes’ so we’re better able to address them.
And for this to happen, we need humility (not hubris), we need creativity and honesty and — if we are to work together– we need trust.
Here are a few other key readings on decolonisation:
For some reason – unlike our health counterparts — nutrition
professionals tend to shy away from research and action on the commercial
determinants of (mal)nutrition. They don’t
want to be involved in polarizing discussions on the role of the private sector
in nutrition.
A big part of the problem is the way the narrative is
shaped. We constantly hear clichés like
“the private sector should be part of the solution”, or simplistic questions
like “how do we work with the private sector?”.
A good start is probably to ban the phrase “private sector”. It’s just not
helpful. There are many forms of private business, including many small
companies who are trying to improve access and affordability to healthy diets. We
need to do better in differentiating those whose products and practices harm nutrition
from those who (actually or potentially) support good nutrition. The former include the ultra-processed food
and beverage industry which controls much of the global food system. They want
to be loved by the nutrition community, so they target influential individuals,
organizations and conferences and woo them in various ways. Adapted from Big
Tobacco, this corporate playbook has been described and used many times. Being
seen to be part of the nutrition community is huge as it confers tacit approval
of actions – a soft-power ‘get out of jail card’ that reduces the pressure to
change damaging products and practices.
And these tactics clearly work.
The nutrition community has made progress in differentiating
good and bad corporate behaviors and even ranking them. Much of this however draws on statements of
intent, rather than action on the ground.
There are different sets of principles that define good (pro-nutrition) behaviour.
But what’s missing is clarity and consensus on what this looks like in
practice, where the red
lines are, and the implications of crossing them.
This is not trivial.
We currently have a divide between some who believe that it’s perfectly
fine to ‘talk to anyone’ and others (myself included) who believe that actions
need to precede words. The ‘talk-first’ group think they can persuade
malnourishing companies to change their ways – as if they were somehow still not
clear on what to do. The ‘walk-first’
group believe it’s perfectly clear to everyone what’s needed, it just needs to
be done – or at least, there needs to be clear, tangible, independently
verifiable progress first. This needs to be large-scale – it’s just not good
enough to have a few showy small-scale CSR projects dotted around, here and
there. Boutique projects and the media
froth they generate are distractions at best. At worst, they’re dangerous side salads
that confer legitimacy on core business practices that may run in a very
different direction.
Malnutrition is a large-scale problem, it needs large
companies to act at large-scale, in the long term, to be seen to be serious.
This year we have not one but two big talking events – the UN Food Systems Summit (UNFSS)
and the Nutrition
for Growth Summit. The rules for engagement in these summits are not
entirely clear. I have been told there are guidelines but they’re not visible
on the web. There is a Private Sector Guiding Group for the UNFSS but again – it’s
not clear who is in this group, or whether it’s open to anyone.
In the various consultations in different Action Tracks for
the Summit there has been a lot of discussion about the importance of enabling
environments, trust and responsibility. On 23 November, the UN Special Envoy, Agnes
Kalibata stated: “One of
the most broken pieces of our food system is our trust in each other. There
isn`t a high level of trust in the system right now, and that is preventing us
moving forward.”
She’s right — it’s crystal clear that many stakeholders see
trust as a big issue.
The UNFSS has put out a call for game-changing solutions. One
that would go a long way to rebuild trust would be an unequivocal position on
the part of the UNFSS regarding the role of the ultra-processed food industry
in the challenge of addressing malnutrition. In general terms, and specifically
with regard to the Summit process.
In his 2019 book “Upheaval: How Nations Cope with Crises and Change”, Jared Diamond starts by interrogating the word ‘crisis’. Coming from the Greek noun ‘krisis’ and the verb ‘krino’ there are several meanings — to separate, decide, a turning point. Crises differ in terms of the way they emerge, their scale, duration, and impact. Some come as a shock, some are slow-burn — though in reality this distinction may be blurred once we look below the surface.
The COVID-19 pandemic is a sudden-onset crisis, while climate
change is slow-burn (albeit linked to increasing shocks like floods and
droughts). The biggest cause of global ill-health and premature mortality – malnutrition
— is also slow-burn. All three crises are
massive in scale, they overlap and interact, and they share many drivers. In
2019, a Lancet Commission delivered an incisive analysis of the global syndemic of obesity, undernutrition, and climate change. This was a year
before the pandemic. COVID-19 has since added another crisis into this toxic mix.
Crises heighten our awareness of time, and they generate new
understandings or worldviews, often elevating neglected issues to centre-stage.
Equity is one such issue.
The COVID-19 pandemic not only exposes inequities of different forms,
it amplifies them. We have seen this clearly in
the experience of Black, Asian and Minority Ethnic (BAME) communities in the UK
and elsewhere, who are disproportionately exposed to the virus, and more likely
to become seriously ill or die. A similar situation plays out with regard to climate
and malnutrition crises. Syndemics are fuelled by inequity.
Equity was the central theme of the 2020
Global Nutrition Report. The introductory chapter succinctly unpacked the
concepts of inequity and inequality, highlighting the core ingredients of unfairness,
injustice and social and political exclusion.
But we also need to take account of another dimension – time. What we do (or don’t do) now — as individuals,
organizations and governments – has immense implications for future
generations.
This is the subject of a powerful new book by Roman Krznaric “The Good Ancestor: How to Think Long-term
in a Short-term World”. While many activists are driving a decolonization
agenda in global health, Krznaric argues that we have also colonized the future.
Starting in the 18th century, Britain colonized Australia,
considering it to be ‘terra nullius’ (‘nobody’s land) ignoring indigenous
peoples’ claims. We are now behaving in
a similar way with time. Political and economic systems consider the future to
be tempus nullius (‘nobody’s time’). Our time horizons have collapsed
inwards, driven by short-term dopamine-triggered feedback loops.
Krznaric distinguishes between the marshmallow brain —
routinely hijacked by the digital distraction industry that has weaponized
smartphones and social media platforms to steal time – and the acorn brain,
that thinks long-term, considering the intergenerational consequences of
actions taken today.
His analysis of intergenerational injustice and the ‘dark art of
discounting’ is compelling. As a method for weighing up the costs and benefits
of investment decisions over different time spans, discounting has spread from
finance into many spheres of development, including public health and
climate-related policymaking.
Why, Krznaric asks, are the lives and well-being of future
generations considered to be of ever-declining value? Using a ‘progressive’ 1.4% discount rate, adults
alive two generations from now would be assigned the value of half a human
today – an ‘iconic expression of the colonization of the future’. Why isn’t the welfare of a child born 100
years from now treated as equal to the welfare of a child born today? Are we to accept that future generations will
continue to be disenfranchised, like slaves and women in the past?
Intergenerational inequity plays out in different ways. Politically, it came to the fore, for
example, in the 2016 Brexit referendum, when young people (overwhelmingly
pro-Remain) accused the older generation (overwhelmingly pro-Leave) of stealing
their futures.
So, what does this have to do with nutrition?
A lot.
A growing body of research in the last few decades has shone a
light on the way in which malnutrition persists through the life cycle – and even
across generations. Epigenetics
is showing that what we do now has major implications for the health of future
generations. A recent
review states:
“Early insults during critical
periods of brain development, both pre- and postnatal, can result in epigenetic
changes that may impact health and behavioral outcomes over the lifespan and
into future generations. There is ample evidence that these early stages of
brain development are sensitive to various environmental insults, including
malnutrition, childhood trauma and drug exposures. The notion that such
changes, both physiological and behavioral, can also carry over into subsequent
generations has long been recognized, especially in the context of experimental
studies. However, epigenetic mechanisms capable of explaining such phenomena
were not available until relatively recently.”
Nutritional disadvantage, driven by inequitable factors and
processes, can last for many decades.
Meanwhile, as we continue to learn more about long-term
consequences, the ultra-processed food industry continues to exploit the short-term,
addictive and impulsive traits of our marshmallow brains — one of the main
reasons why obesity has rocketed in the last two decades. In evolutionary
terms, we’re still very close to hunter-gatherers who were adapted to consuming
food whenever and wherever they could.
What used to be a survival mechanism to bridge over times of scarcity, however,
has become a maladaptation to the obesogenic environments we now live in.
What to do?
Following the Global Nutrition Report’s call, we need to develop and
invigorate a pro-equity nutrition agenda that includes intergenerational
justice.
Security is a start point. How can anyone ‘think long’
or plan for the future if they cannot even nourish their families today? Food,
health and nutrition security are foundational pillars for building a future –
at all levels.
Second, nutrition researchers and activists need to become politically
adept in analysing and challenging political and governance systems that colonise
the future. For too long, the nutrition community considered politics
and political economy as beyond their remit. We have a special challenge
given that the full benefits of addressing malnutrition will take many more
years than a politician’s term in office.
Third, institutional mechanisms that ‘look long’ and consider
interests of future generations need cultivating – especially youth
movements, such as the Scaling
Up Nutrition (SUN) Youth Leaders for Nutrition. A Lancet Planetary
Health commentary,
released alongside International Youth Day last week, argues: ‘It is time to democratise [planetary health], balance the
asymmetrical power structures, and leverage
fearless voices challenging the status quo’. The authors outline a pragmatic roadmap based on three
pillars: governance structures enabling young people’s participation, funding
that supports inclusion and compensation of young people from all backgrounds,
and capacity building for young people.
Another example of long-termism, as highlighted in the Lancet
syndemic commission report, is the Iroquois concept of ‘seven generation
stewardship’. This urges the current generation to live and work for the
benefit of the seventh generation into the future. To this end, the Commission
proposed the establishment of a ‘Seven Generations Fund for Traditional
Peoples’ Science’.
Nutrition advocacy that emphasizes the foundational
aspects of nutrition, and its central role within holistic strategies for
achieving the Sustainable Development Goals
will be more important than ever. In this context, #BuildBackBetter has become a
bit of a cliché in 2020. Many also question use of the word ‘back’. Why go back to economic systems that target
short-term gains, and profit over people? Why not go forward?
The SDGs rightly focus on sustainability and on equity – leaving no-one
behind. In this context, the title of the postponed ‘Nutrition for Growth’ summit is
looking ever more dated. Yes, we know that $1 invested in nutrition generates
$16 in returns. The economic investment case needed to be made a decade ago,
and it’s been made. Now we need to make the case in terms of nutrition’s
pivotal role as a driver of sustainable and equitable development. ‘For Growth’
is just not a compelling rationale any more. The world has changed.
Finally, we face a challenge of public perception that can
perhaps be best illustrated by a mythical fable about frogs and hot water (don’t
try this at home!). If you drop a frog into boiling water it hops straight out.
If you drop a frog into tepid water and heat it to boiling, it will not react
until it’s too late. The COVID-19 pandemic is a rapid-onset global emergency
that has generated an unprecedented sense of crisis and a large-scale response.
The climate and nutrition crises, on the other hand, are slow-burn crises that proceed
incrementally, month by month. They kill
many more people than COVID-19 but they do not generate a sense of crisis that
leads to action on the scale and intensity required. It’s reflected also in the
terminology – the notion of climate ‘change’ is a little like referring
to an earthquake as a ‘land movement’!
So, the overarching challenge is to generate a sense of urgency that leads to concerted large-scale action. One opportunity lies in showing the connections (through data and research) within the syndemic. During the southern African HIV epidemic in the 2000s, a similar approach was taken with nutrition, following research that showing that antiretroviral therapy did not work well unless people were adequately nourished. A recent example comes from the UK where evidence of the higher risks of COVID-related hospitalization and death of people who were obese led quickly to a strategy (flawed, but a start) to address obesity.
At long last, equity – including transgenerational justice – is central
to the nutrition agenda.
As the COVID-19
pandemic generates waves of impact across the globe, “resilience” is bouncing
back into the development spotlight.
Whether linked to
health (e.g. AIDS, Ebola) or economic (food prices), climate or conflict shocks
and stresses, resilience has come to be seen as a useful organizing principle.
A conveniently fuzzy, all-embracing, cross-sectoral goal around which we can all
align.
There are many
definitions out there. Most refer to the ability – in the face of a shock or
stress — to recover or bounce back to a past state. A type of buoyancy or toughness in the face of adversity — the capacity to weather the storm, to
cope. The Intergovernmental Panel on Climate
Change, for example, defines
resilience as the ‘ability of a system and its component parts to
anticipate, absorb, accommodate, or recover from the effects of a hazardous
event in a timely and efficient manner’.
In the face of
COVID-19, at an individual level, resilience is ultimately the ability to
survive. For households, it’s the ability to withstand multiple social and
economic impacts.
Alongside the
return of resilience, we see another emerging discourse that argues for the
need to jettison business-as-usual in a post-COVID world. We need to create a “new normal”. This sounds
very like transformation — quite different to coping.
So, can these two
goals – resilience and transformation – actually co-exist?
But first, even
before we ask questions about resilience, we need to consider resistance.
The front-line of resistance to a new virus like SARS-CoV-2 is an individual’s
immune system. We can go further back to ask why s/he was exposed to the virus
in the first place — was she working or living in an environment in which she
had more contact with potential carriers? Was she in control, could she reduce
the risk of exposure? If her ability to avoid exposure – her resistance — is
overwhelmed and she becomes infected, then we’re in the realm of resilience.
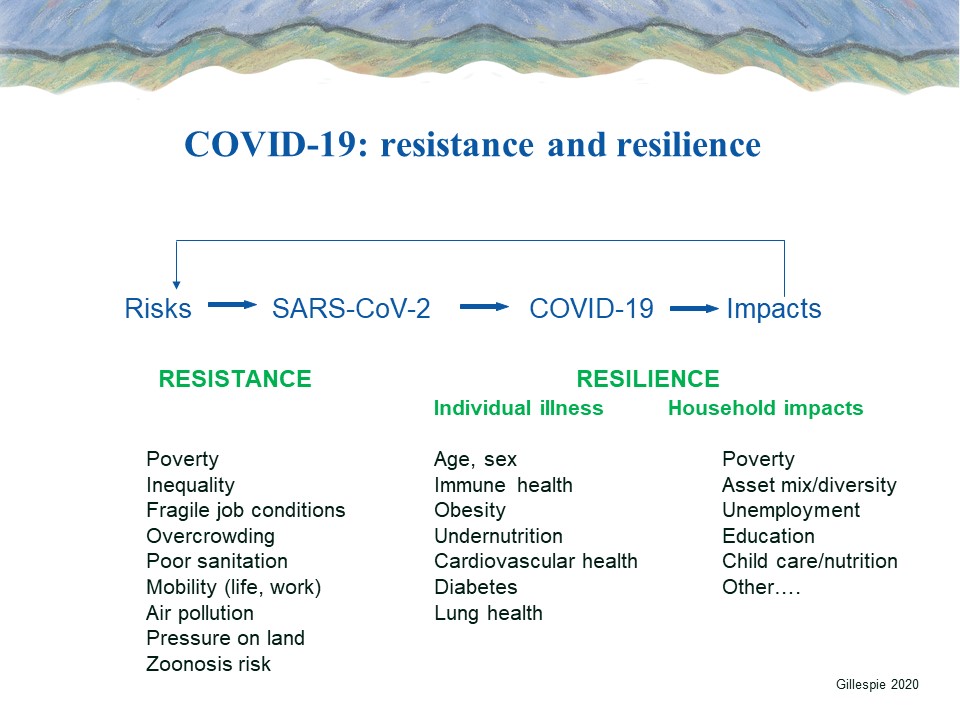
In 2003, in the
early years of RENEWAL, we conceptualized both resistance
and resilience in the context of AIDS epidemics to help understand the
different layers and waves of HIV risk and AIDS impacts. In the top left
quadrant (of the diagram below) we can see the different drivers of risk of
exposure to the virus, from macro to micro.
In the top right quadrant, we can see the waves of impact, from micro to
macro. The bottom half shows potential
responses – resistance to the left, resilience to the right.
As we learn more
about COVID-19, we can develop similar maps to help situate a comprehensive
response. Here’s a simplified illustrative
version, including potential key factors (some as yet unproven):
Much has been
written about resilience in recent years. In May 2014, IFPRI convened an
international conference “Building Resilience for Food and Nutrition Security”
in Addis Ababa, Ethiopia that led to a book
of key papers.
Where is agency?
One criticism of
resilience in the past has been its perceived inability to capture issues of
power, agency and social justice. It’s seen as an apolitical concept that is
not necessarily pro-poor. It is quite conceivable, for example, for a household
to demonstrate resilience (using a certain metric) but for this to entail major
costs. A household may remain “food-secure” in the face of climate shocks or
seasonal stresses, but there may be a big price to be paid (e.g. to the nutrition
and health of women working dawn til dusk transplanting rice, and/or to young
children who are not adequately cared for during peak labour demand).
Clearly there are
potential trade-offs. We need to ask questions about equity, about the cost
of resilience, and who pays? We need to consider scale (individual,
household, community etc) and timeline (e.g. does resilience endure?).
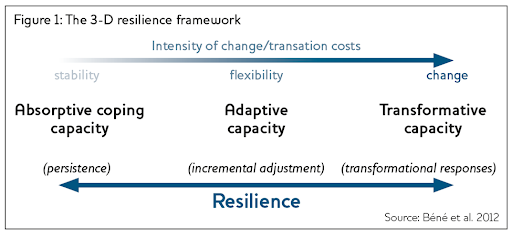
Pelling (2011), for example, argues that the notion
of resilience as “buffering” is too limited as it simply reinforces the status quo. Bene et al (2012) suggest a more organic way to bring
power and agency into resilience thinking is to incorporate them directly into
the conceptualization, as per their “3-D framework”.
Beyond the
limited notion of the capacity to cope by absorbing shocks (on the left), there
is the capacity to adapt, and even to transform. At a systemic level, this refers to a
fundamentally new food or health system.
Agency, power and
politics are thus captured in this framework. We can also see how the ability
to absorb a shock ensures stability, which in turn provides the potential for
incremental adjustments and even transformational change.
We could apply such
a framework to individuals, households and communities — and we could apply it
to health and food systems. Bringing in the related concept of vulnerability,
we can see how certain food systems — in which wild animals, domestic animals
and humans are in close proximity in wet markets — are vulnerable
to zoonotic emergence. The virus crossed species and now it’s crossing
entire systems. Emerging from a food system, it has gone on to overwhelm health
systems, and to undermine global economic systems in a way that’s not been seen
for more than a century.
Societies and
economies will survive — in some form. In the aggregate, they are
resilient. But the COVID-19 pandemic is
exposing and amplifying many forms of inequity. We need to differentiate
actions and impacts within households and health or food systems and ask
questions about the cost of resilience, and who actually pays?
In the UK, for
example, it is front-line health workers who — day after day, separated from
their own families for weeks on end — put their lives at risk to keep people
alive. The resilience of the health system (in this case, the NHS) derives from
the actions of these individuals. They are paying the price of resilience — not
the politicians who, for years, have argued against raising their wages, and
who dithered for weeks before responding to the pandemic.
In sum, resilience
can be a useful common goal across sectors and systems — so long as it is
treated comprehensively, and so long as it includes an analysis of equity. And
it is possible to strive for resilience and to pave the way for transformation
into a more sustainable, more equitable future. These two goals are not mutually
exclusive. But it will require actions that strengthen all three components of
resilience (absorptive, adaptive and transformative) together, at multiple
levels (individual, household, community).
And what can we learn from the response to the AIDS pandemic?
By Stuart Gillespie and Alan Whiteside
The COVID-19 pandemic is generating multiple waves of unprecedented global impacts. Epidemics in Europe and the United States are currently in their exponential growth phase, following declines in infection rates in China, South Korea, and Japan.
We have not yet seen major epidemics take off in South Asia, Latin
America and Africa south of the Sahara—where governments, health and food systems,
communities, and households have limited capacity to respond. But we do know
they will take off. Very soon.
In the first decade of this century, we learned a lot about how the
AIDS pandemic interacts with food and nutrition security—including how food
insecurity could heighten the risk of exposure to HIV in several ways. We learned
more about the upstream risks, including how undernutrition weakens the ability
to cope with HIV infection, leaving those with HIV less able to delay and
resist the worst effects of opportunistic infections that can kick in several
years after acquiring the virus. And we learned about the different types of downstream
impacts of HIV and AIDS on households and communities in hard-hit areas—and the
types of responses that mitigated these impacts.
AIDS epidemics are long-wave phenomena. In fact, there have been several
waves: The first wave of HIV infection in the 1980s was followed by increased
incidence of opportunistic infections and, several years later, by the third
wave of AIDS disease and death. Beyond this, depending on a host of variables,
there was a fourth wave encompassing a stream of economic and social impacts at
the household, community, and national levels. With regard to COVID-19, the
timeline is compressed significantly, with three waves—of infection, illness,
impact—the first two separated by just a week or two.
We are among the contributors to a considerable body of work on
the HIV and AIDS epidemics and food and nutrition. In our view, there is much
to learn from AIDS as we confront COVID-19—but there are also critical
differences. One is that, wherever they occur, COVID-19 epidemics are massive short-wave
shocks that will generate long-wave impacts. These impacts will manifest in
different ways in different contexts for many years to come. How we respond to
the first wave will determine the capacity of health and food systems to cope,
to keep people alive, and to buffer impacts on livelihoods and the food and
nutrition security of people who depend upon them.
In this post, we discuss some important questions about food and
nutrition, and about equity, as the pandemic begins to accelerate in lower
income countries.
Who
is at greatest risk?
We don’t know enough about what drives personal risk
of a severe infection, although age and certain preexisting conditions are key
factors in the north. Populations in the south are, on average,
significantly younger than those in Europe and North America, but it is the
elderly who are likely to be at highest risk.
We
do know a lot in general about nutritional status and immune health. Half a century
ago, the term “nutritionally
acquired immune deficiency syndrome” (NAIDS) was first used. Malnourished individuals are more likely to
have severe COVID-19 symptoms, possibly requiring hospitalization. These vulnerabilities
can be driven by undernutrition or by overweight and obesity. Intensive care data from the United Kingdom
suggest that obese adults are at higher risk of severe symptoms from the
disease. The immune systems of people with obesity are chronically activated to
respond to cellular damage caused by inflammation. Physically, obese adults also
have a harder time dealing with pneumonia, as excess weight can compromise the
ability of lungs to take in oxygen. Obese adults are more likely to have poor
cardiovascular health and less likely to be physically active—both factors
potentially compromising immune health. And there are other possible
interactions with non-communicable disease such as diabetes that are being
explored as more data become available. COVID-19 also has important implications for people currently living with HIV
and/or tuberculosis, including the critical need for testing and adherence to
treatment protocols.
Where
do they live?
COVID-19
is a respiratory disease that spreads rapidly in overcrowded contexts where
many people are in frequent close contact, especially in insanitary conditions—for
example, an urban slum or a refugee camp. The
virus is 2-3 times more infectious than normal flu.
Urban
slum populations are more likely to be sedentary, and to be exposed to air
pollution that both adversely affects lung health and the ability to deal with
severe respiratory disease. Urban populations are also more likely (than rural)
to consume ultra-processed
foods which are widely available
and known to significantly increase the risk of obesity and other
non-communicable diseases.
We don’t know
much yet about the ability of the virus to thrive and spread in tropical environments.
Ecological niche models—developed to project
monthly variation in climate suitability of COVID-19—suggest the virus may
prefer cool and dry conditions (similar to its predecessor SARS-CoV), though this
remains a hypothesis.
Expected impacts
Given the links between COVID-19
epidemics and the livelihoods, food and nutrition security of the poor in
lower-income countries with relatively weak healthcare systems, we can expect the
disease will have serious impacts. As with the AIDS pandemic, the
conditions exist for vicious cycles of upstream risk and downstream effects,
particularly for the ultra-poor.
Most
immediately, COVID-19 has already generated a massive global economic shock. In
general, economic downturns and recessions (whatever the cause) hit the poorest
households hardest via numerous pathways (higher food prices, less purchasing
power, reduced ability to stockpile, higher risk of losing jobs, lack of safety
nets, ability to access and afford treatment and care, etc.). Workers from poorer
households cannot afford to take time off work if they are feeling unwell. There
are multiplier effects—a recent multi-country study in Africa south of the Sahara and South/Southeast Asia found
that responses to health
shocks by people in poverty who
did not have health insurance or access to healthcare included distress sales
of assets and widespread exploitation by informal moneylenders. This was also a
common
response to AIDS shocks.
Second, COVID-19 is already having a
major impact on supply chains and logistics, both for producers and consumers—as evidenced
by closed borders, national lockdowns, and the reduction in air traffic. We
believe this will have many adverse effects on food and nutrition security,
especially in the global south.
Finally, a wave of deaths among grandparents and the elderly may
significantly impact the care of young children, especially among the poor
reliant on informal sector jobs. This in turn may raise their risk of becoming
malnourished.
How to respond?
UNAIDS have just released a new publication, Rights in
the Time of COVID-19: Lessons from HIV for an effective, community-led response. It has seven
key takeaways: 1) engage communities, 2) combat stigma, 3) test, test, test, 4)
help people protect themselves, 5) clarify evidence-based restrictions, 6)
country cooperation, and 7) the crucial need to support and protect health
workers.
Another overarching lesson from the AIDS crisis was
the need to engage actors from many disciplines in a comprehensive
multisectoral response that revolved around strengthening community and state
capacity to respond, both effectively and sustainably. The same will apply to COVID-19. A day is a long time in this pandemic,
as everything is moving so fast—but we have to apply these lessons now.
Turning to the health system and the immediate response, proven preventions
being deployed in the global north comprise social (or physical) distancing, testing,
tracking, and quarantines. As a March 26 Economisteditorial
observed: “Without a campaign of social distancing, between 25% and 80% of a
typical population will be infected. Of these, perhaps 4.4% will be seriously sick
and a third of those will need intensive care. For poor places, this implies
calamity.” On the same day, Imperial College, London published a paper on the
global impact of COVID-19 and strategies for mitigation and suppression, employing
modeling data from 202 countries. Doing nothing to
combat the virus would lead to around 40 million deaths this year, the report
said—a higher death toll than four decades of the AIDS pandemic. Social distancing
could halve this, but will require a monumental effort in urban contexts
in the global south. Health systems could be quickly
overwhelmed.
Beyond
health system responses, there’s a critical need to develop and to strengthen
social protection systems. In the early 2000s, social protection systems were AIDS-proofed.
We now need COVID-proofing to protect the most vulnerable and to dampen viral transmission.
Finally, COVID-19 presents major issues for food systems. As with all responses, the state needs to play a leading role. But the crisis also raises questions about the role of the private sector in buffering food and nutrition impacts on poor households, especially in urban areas. Seven years ago, the eerily titled paper “Profit and Pandemics” spotlighted the products and practices of transnational food companies and the massive damage being wrought by ultra-processed foods in the global south. Since then, we’ve learned a lot more about the harm these foods cause to nutrition and health—harm that may translate into greater risk of severe COVID-19 disease for millions. Just as they were in the era of AIDS, human rights advocacy and activism will be key in turning back the COVID-19 epidemic, and to defining a new future that goes well beyond “business as usual.”
Stuart Gillespie is a Senior Research Fellow with the International Food Policy Research Institute, and founder of the Regional Network on AIDS, Livelihoods and Food Security (RENEWAL), 2001-2010.
Alan Whiteside is CIGI Chair in Global Health Policy, Wilfrid Laurier University and Balsillie School of International Affairs, Canada. In 1998 he founded the Health Economics and HIV/AIDS Research Division at the University of Natal, South Africa (HEARD).
This website uses cookies to improve your experience. We'll assume you're ok with this, but you can opt-out if you wish. Cookie settingsACCEPT
Privacy & Cookies Policy
Privacy Overview
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorized as necessary are stored on your browser as they are essential for the working of basic functionalities of the website. We also use third-party cookies that help us analyze and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these cookies. But opting out of some of these cookies may have an effect on your browsing experience.
KOYA and any person connected to the organisation do not collect any data from website users. We do not nor will we ever share any information you share with us but any other method.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Any cookies that may not be particularly necessary for the website to function and is used specifically to collect user personal data via analytics, ads, other embedded contents are termed as non-necessary cookies. It is mandatory to procure user consent prior to running these cookies on your website.